Beyond Hand Washing: The Complete Guide to Types of OCD
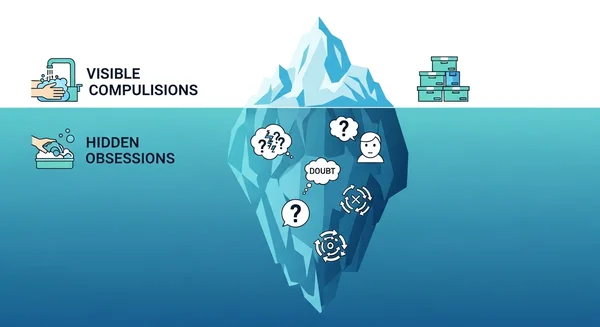
If you asked the average person to describe Obsessive-Compulsive Disorder (OCD), they might picture someone washing their hands repeatedly or arranging pencils in a perfect row. But if you are living with intrusive thoughts, doubts about your relationship, or a paralyzing fear of harming someone, these stereotypes don't just feel inaccurate—they feel isolating.
The reality is that OCD is not a "one-size-fits-all" condition. It is a complex spectrum of "dimensions" that manifests differently for everyone. You might have zero desire to clean, yet spend hours mentally reviewing a conversation you had three years ago.
This guide explores the various types of OCD, from the well-known categories to the "hidden" subtypes that often go undiagnosed. We will help you understand the patterns, clarify your symptoms, and explore our OCD test online to gain better insight into your specific situation.
Is It Just a Quirk or OCD? Understanding the Core Categories
Before diving into the specific subtypes, it is crucial to distinguish between a personality quirk and a clinical condition. Many people say, "I'm so OCD about my coffee," but true OCD is not about preference; it is about distress.
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders) categorizes OCD based on the presence of obsessions (unwanted, intrusive thoughts) and compulsions (repetitive behaviors performed to neutralize the anxiety caused by those thoughts).
The "Dimensions" of OCD: Why It's Not Just One Thing
Clinicians often refer to the types of OCD as "symptom dimensions." This is because symptoms rarely stay in one neat box. You might primarily deal with contamination fears but also experience checking behaviors when you leave the house.
Understanding these dimensions helps you realize that your internal experience—even if it seems "weird" or unrelated to cleaning—is valid and recognized by mental health professionals.
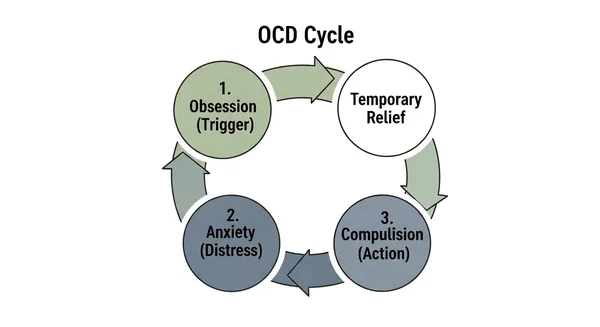
Obsessions vs. Compulsions: The Cycle Explained
To identify your type, look for the cycle. This loop is the engine that drives all forms of the disorder:
-
Obsession (The Trigger): A "what if" thought spikes your anxiety (e.g., What if I left the stove on and the house burns down?).
-
Anxiety (The Feeling): An intense wave of distress, panic, or a feeling of "incompleteness."
-
Compulsion (The Fix): You perform an action to relieve that anxiety (e.g., Checking the stove three times).
-
Temporary Relief: You feel better for a moment.
-
Repetition: The brain learns that the compulsion "saved" you, so the next time the doubt returns, the urge to check is even stronger.
The 4 Most Common Types of OCD Explained
When researchers and doctors discuss "what are the 4 types of OCD," they are generally referring to the four main symptom clusters identified in clinical settings. These represent the most frequent ways the disorder presents itself.
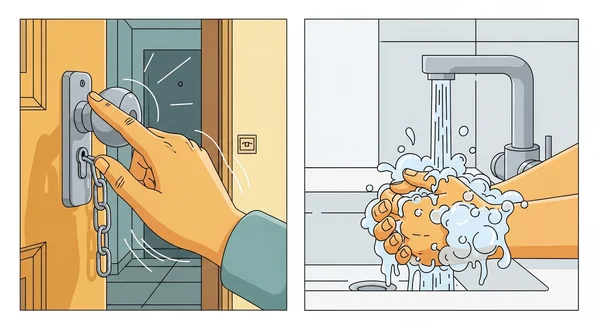
Contamination & Cleaning (The "Washer")
This is the most recognized form of OCD, but it goes deeper than just a fear of germs. It often involves a magical thinking component—the idea that if you are "contaminated," something bad will happen to you or your loved ones.
Common Signs:
- Excessive hand washing or showering until the skin is raw or bleeding.
- Creating "clean" and "dirty" zones in the house (e.g., "outside clothes" cannot touch the bed).
- Avoiding public spaces, door handles, or shaking hands.
- Mental Contamination: Feeling "dirty" emotionally after interacting with someone who treated you badly.
Motivation: Usually a fear of illness, death, or spreading harm to others.
Checking & Doubting (The "Checker")
This dimension is driven by pathological doubt and an over-inflated sense of responsibility. You might trust your eyes less than your fear. Even if you saw the door lock, your brain sends a signal saying, "Are you sure? What if you blinked and missed it?"
Common Signs:
- Repeatedly checking locks, stoves, appliances, or windows (often in a specific number pattern).
- Retracing driving routes to ensure you didn't hit anyone (Hit-and-Run OCD).
- Checking your body for signs of illness (hypochondria overlap).
- Mentally replaying conversations to check for mistakes or offenses.
Mini-Checklist: Do I have Checking Symptoms?
-
Do you take photos of appliances to prove they are off?
-
Do you feel a "nagging" physical sensation that something is unsafe until you check?
-
Does checking once never feel like enough?
-
Do you ask others for reassurance? ("Did I lock that?")
Symmetry & Ordering (The "Arranger")
Unlike the "Checker" who usually fears a specific disaster (fire, theft), the "Arranger" is often driven by a sensory need for things to feel "just right" (Not Just Right Experience, or NJRE). If items are misaligned, it creates a visceral sense of incompleteness or a psychological itch that cannot be scratched until the environment is fixed.
Common Signs:
- Aligning books, canned goods, or clothes by color, size, or direction.
- Needing to walk through a doorway "correctly" or tap things an even number of times.
- Rewriting lists or emails repeatedly until the handwriting is perfect.
- Feeling intense physical tension or "wrongness" when symmetry is disrupted.
Intrusive Thoughts & Taboo Themes (The "Rumination")
This category involves obsessions without visible compulsions. Historically called "Pure O," the compulsions here are mental—like praying, counting, or arguing with the thoughts in your head. The themes are often violent, sexual, or blasphemous, causing immense guilt and shame.
Common Signs:
- Unwanted images of hurting a loved one or a stranger.
- Intrusive sexual thoughts about children, family members, or religious figures.
- Fears that you are secretly a "bad" person or a monster.
- Mental Rituals: Reviewing the thought to prove you don't like it, or trying to "cancel out" a bad thought with a good one.
Motivation: A desperate need to gain certainty about one's moral character or safety.
The "Hidden" Subtypes: OCD You Might Not Recognize
Beyond the "Big 4," there are rare types of OCD and specific subtypes that are frequently misunderstood. If you haven't seen your symptoms listed above, you may find them here.
Myth vs. Reality: Clearing the Confusion
Before looking at specific hidden types, let’s address common misconceptions that keep people from recognizing their symptoms.
| Myth | Reality |
|---|---|
| "I don't do rituals, so it's not OCD." | Compulsions can be entirely mental (counting, praying, replaying memories). |
| "Thinking about violence means I want to do it." | OCD thoughts are "ego-dystonic," meaning they are the opposite of what you want and value. |
| "I just worry a lot about my relationship." | If the worry is cyclical, demand absolute certainty, and involves checking, it may be ROCD. |
Pure O (Purely Obsessional): The Invisible Struggle
"Pure O" is a slightly misleading term because rituals still exist—they are just invisible to the outside world. If you have this subtype, you are likely exhausted from constant mental warfare. You might spend hours analyzing your feelings, bodily sensations, or memories to get reassurance.

Relationship OCD (ROCD): Anxiety in Love
ROCD attacks your most important connections. It is not the same as standard relationship doubts; it is a relentless loop of questions like, "Do I really love them?" or "Are they right for me?"
Key Indicators:
- Constantly comparing your partner to others or an imagined "ideal."
- Fixating on a partner’s minor physical flaws (nose, laugh, etc.) to the point of distress.
- Seeking constant reassurance from friends that your relationship is "normal."
Harm OCD & Scrupulosity: Fear of Loss of Control
Harm OCD involves the terrifying fear that you will snap and hurt someone, despite having no desire to do so. Scrupulosity (Religious/Moral OCD) involves an obsession with whether you have sinned, offended God, or violated a rigid moral code.
Crucial Distinction: People with these types of OCD are often the least likely to act on these thoughts because the thoughts contradict their core values.
Hoarding Disorder: A Related Condition
While the DSM-5 now classifies Hoarding Disorder as a distinct condition, it was long considered a subtype of OCD. Many people with OCD also struggle with hoarding behaviors due to a fear of throwing away something "important" (information or items) or a need for emotional completeness.
Identifying Your Patterns (Self-Assessment)
Reading about these classifications can be overwhelming. You might feel like you fit into three different categories, or you might see parts of yourself in the "Hidden" subtypes that you never realized were symptoms.
Recognizing your specific types of OCD is a powerful step toward management. It shifts the narrative from "I am crazy" to "I have a recognized pattern of symptoms."
Why Recognizing Your Subtype Matters
Knowing your primary subtype helps in therapy. For example, "Symmetry" OCD might require different exposure exercises than "Scrupulosity." However, self-reflection can be difficult when anxiety is high.
Take the Next Step: Educational Symptom Checker
If you are unsure where your symptoms land or how severe they might be, using a structured OCD screening tool can help clarify the confusion. It can organize your experiences into data that is easier to understand.
- Gain Clarity: See which symptom dimensions are most prominent for you.
- Prepare for Support: Use the results to start a conversation with a professional.
- Safe Exploration: No judgment, just insight.
Note: This tool is for educational purposes and self-reflection only. It is not a clinical diagnosis.
Overlapping Symptoms: Can You Have Multiple Types?
The short answer is: Yes.
It is very common to have "mixed" OCD. You might be a "Checker" who also deals with intrusive thoughts. Furthermore, types of OCD can morph over time. You might have struggled with contamination fears as a child, only to develop perfectionism and symmetry issues as an adult.
The core mechanism—intolerance of uncertainty—remains the same, even if the "theme" of the obsession changes.
Living with Uncertainty: 3 Daily Coping Strategies
While professional treatment is the goal, you need tools to manage the daily struggle. Here are three strategies to help you navigate triggers, regardless of your OCD type.
- Delay, Don't Deny: When the urge to perform a compulsion hits (e.g., checking the lock), try to delay it. Say, "I will check, but I'm going to wait 2 minutes." This builds your "uncertainty muscle" and weakens the urgency over time.
- Label the Thought: When an intrusive thought appears, acknowledge it without engaging. Say, "That is an OCD thought," or "That is a spam email from my brain." Don't open the email; just let it sit in the inbox.
- Practice Self-Compassion: OCD is not a character flaw. Be gentle with yourself on hard days. You are fighting a tough battle, and you deserve credit for trying.
How Are Different OCD Types Treated?
Regardless of whether you have common types of OCD or rarer forms, the gold standard for treatment remains consistent.
The Gold Standard: ERP Therapy
Exposure and Response Prevention (ERP) is the most effective therapy for all types of OCD.
- Exposure: You intentionally face the trigger (e.g., touching a doorknob, having a "bad" thought) in a controlled way.
- Response Prevention: You resist the urge to perform the compulsion (e.g., not washing, not analyzing the thought).
Over time, this teaches your brain that the anxiety is manageable and that the "bad thing" won't necessarily happen.
Medication and Professional Support
For many, a combination of ERP therapy and medication (usually SSRIs) provides the best relief. If your symptoms are interfering with your daily life—work, relationships, or sleep—seeking a professional diagnosis is the most important step you can take.
You Are Not Your Thoughts
Understanding the types of OCD is the beginning of reclaiming your life. Whether you are washing, checking, arranging, or ruminating, the underlying message is the same: your brain is stuck in a loop of doubt.
But you are not your thoughts, and you are not your anxiety. By identifying the specific form your OCD takes, you strip away some of its power.
If you are ready to gain more insight into your patterns, we encourage you to try the OCD test as a starting point for your journey toward clarity and recovery.
Frequently Asked Questions
What is considered the rarest type of OCD?
While data varies, types like Somatic OCD (obsessing over autonomic body functions like blinking, breathing, or swallowing) and purely Existential OCD (obsessing over the nature of reality or the universe) are often reported less frequently than contamination or checking types. However, they may just be under-reported due to lack of awareness.
Which type of OCD is considered the hardest to treat?
Severity is usually more significant than the specific type. However, "Pure O" (mental rituals) can be perceived as challenging to treat because the compulsions happen internally. This makes it harder for a therapist to observe the ritual and intervene during ERP exercises, but it is still highly treatable with the right approach.
Does the type of OCD I have change the treatment plan?
The structure of treatment (ERP) remains the same, but the content of the exposures will differ. A "Washer" will practice touching dirt without washing, while someone with "Harm OCD" might practice holding a knife while cooking to prove they won't lose control. The goal is always to face the specific fear without neutralizing it.
Can overthinking be a form of OCD?
Yes, if the overthinking is repetitive, intrusive, causes distress, and you perform mental "checks" to neutralize the thoughts. This is often the hallmark of the "Rumination" or "Pure O" type. General overthinking (worrying about real-life problems like bills or work) is usually more aligned with Generalized Anxiety Disorder (GAD).
Is it possible for my OCD type to change over time?
Absolutely. This is known as "symptom shifting." It is common for the themes of OCD to change as you age or as your life circumstances change. For example, a new parent might suddenly develop "Harm OCD" focused on their baby, even if their previous symptoms were strictly about organization.